I’ve been studying medicine for 40 years and have treated thousands of patients. I’ve learned you don’t fully grasp the meaning of a diagnosis until you or a family member has lived it.
All healthcare exists on two planes: biology (our bodies) and psychology (how we feel about our bodies). My experience transitioning from a negative to a positive calcium score test gave me new insight into both.
I’ve always been thin and athletic, carrying a self-image of being a “healthy guy.” At 54, I underwent a coronary artery calcium scan and received a score of zero: no detectable calcium in my coronary arteries.
No other risk factors flagged. My identity as “the healthy guy” was reinforced.
Seven years later, I repeated the scan. This time, my score came back at 14, mildly positive on a scale of zero to 1,000.
Even that small number changed my self-perception. A positive score meant I was developing atherosclerosis in my coronary arteries, a process likely occurring throughout arteries in my body.
I reviewed my cholesterol panel, which showed no red flags: total cholesterol 185, HDL 49, LDL 127, ApoB 102. None of those numbers screamed danger.
But given the positive calcium score, the cholesterol values became less important. My body was developing coronary artery disease regardless of how “okay” my panel looked.
In consultation with my doctor, I started a low-dose statin: half of a 5mg rosuvastatin (Crestor) tablet daily. My repeat cholesterol panel was striking: total cholesterol 145, HDL 50, LDL 82, ApoB 72, with a 30–35% reduction in LDL and ApoB. That medication reduced my risk of a major cardiac event by 20–30%.
My perception of being a “healthy guy” was dented. But I was 20–30% less likely to have a heart attack and die, and the peace of mind of knowing I’m slowing down the clogging of my pipes has independent value. Without that scan, I never would have known.
When Blood Work Isn’t Enough
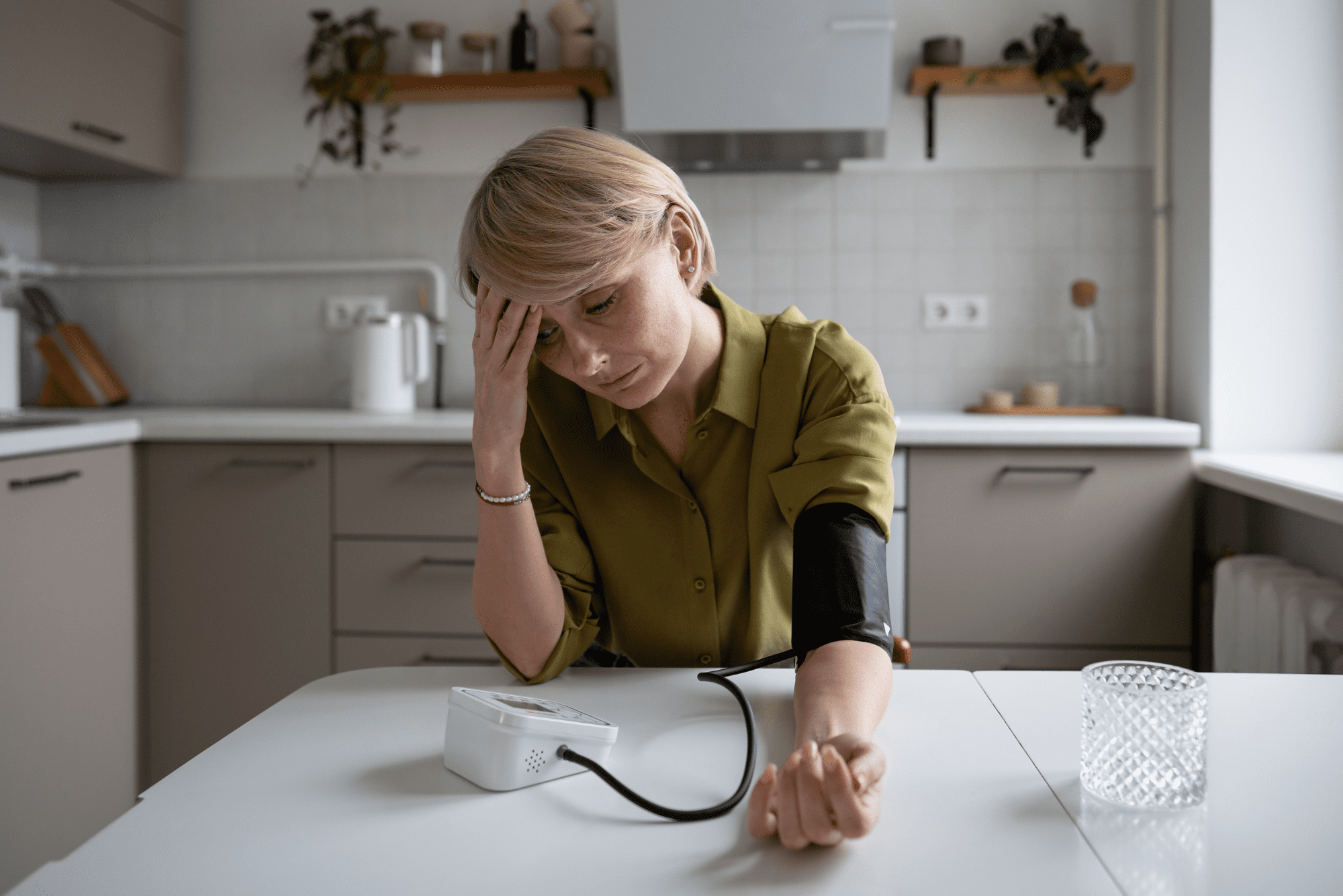
A standard annual blood panel, including HDL, LDL, triglycerides, and (if your doctor orders it) ApoB, gives you a statistical estimate of future risk. If those numbers fall in the normal range, it’s natural to feel reassured.
The problem: Approximately half of all MI patients present with LDL cholesterol levels that are not considered elevated (LDL-C <100 mg/dL). Routine blood work alone doesn’t catch them.
A lipid panel estimates the statistical probability of what might happen; a calcium score test shows what is already happening. The distinction is the difference between a weather forecast and looking out the window. One predicts; the other confirms.
How the Calcium Score Test Works
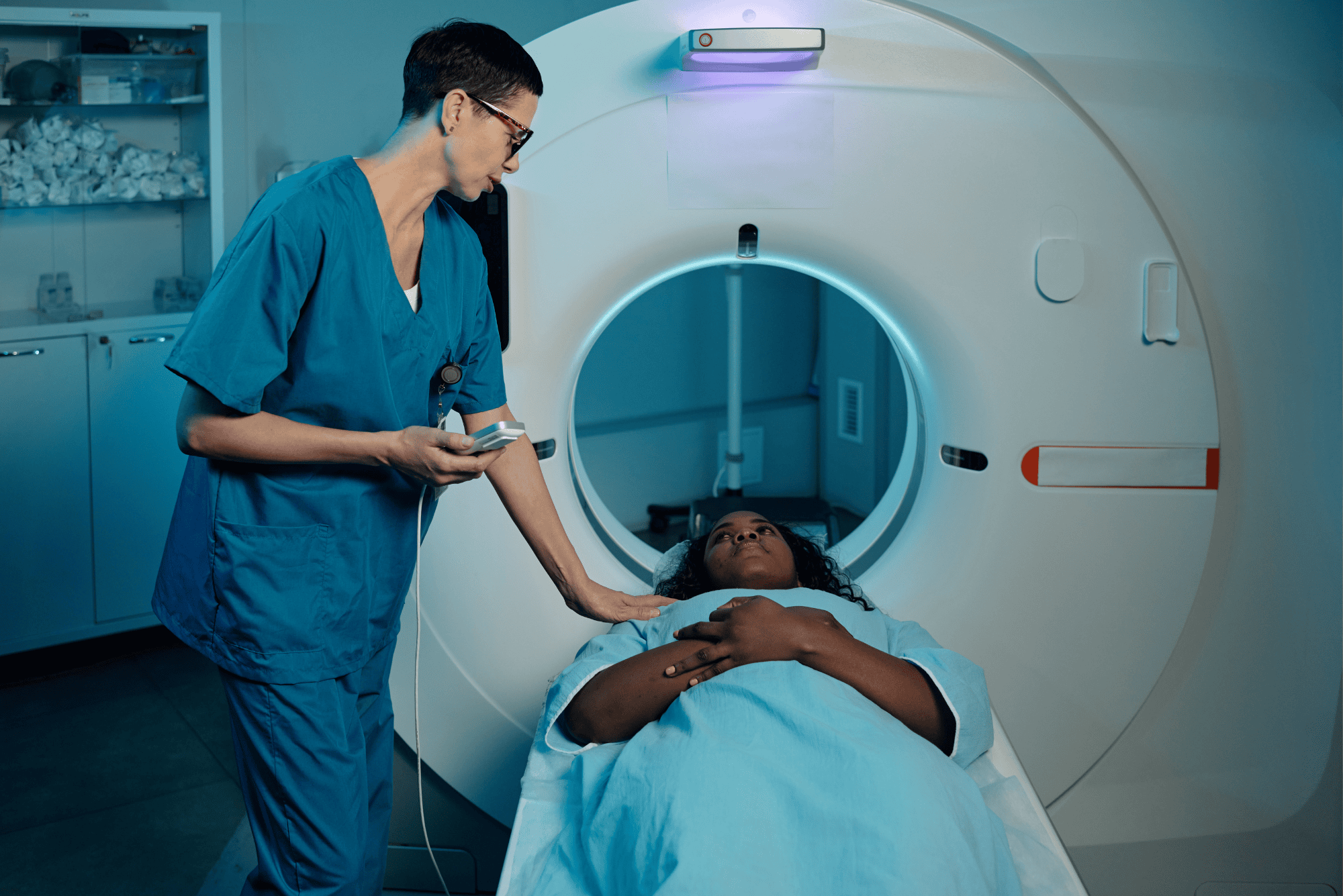
Calcium is radio-opaque, meaning X-rays can’t pass through it. A CT scan (a three-dimensional X-ray) exploits this property to image calcium deposits in the coronary arteries.
The calcium score test is one of the simplest and most informative cardiac screenings available. No IV, no contrast dye, no treadmill. You lie on a table, hold your breath, and in fewer than 10 minutes, you’re done.
The result is a single number, your Agatston score, on a scale from zero to over 1,000.
This screening sits in a unique space. A standard executive physical might include detailed blood work and a physical exam, but few panels directly image the coronary arteries. The scan fills that gap.
What the Scores Mean
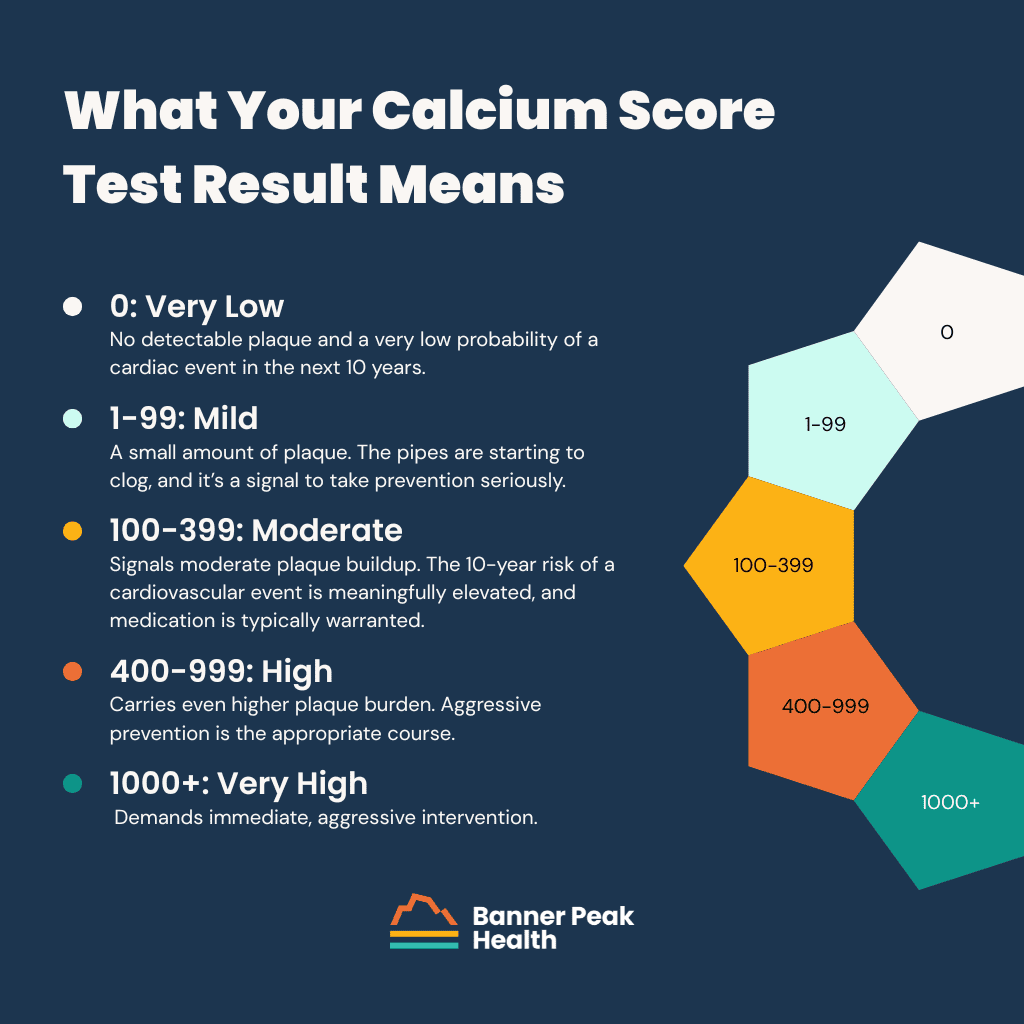
The Agatston score is divided into ranges, each with a different clinical implication:
- A calcium score test result of zero means no detectable plaque and a very low probability of a cardiac event in the next 10 years. This is the best possible outcome. It doesn’t guarantee immunity from heart disease, but it’s strongly reassuring.
- A score of one to 99 indicates a small amount of plaque. The pipes are starting to clog, and it’s a signal to take prevention seriously. Lifestyle modification is the first step. For some patients, this range tips the conversation toward medication, particularly statins. After nearly 40 years of clinical experience with this drug class, the risk-benefit profile of statins remains among the most favorable in medicine, with side effects that are rare and typically reversible (most commonly muscle aches, similar to those with other cardiac medications).
- A score of 100 to 399 signals moderate plaque buildup. The 10-year risk of a cardiovascular event is meaningfully elevated, and medication is typically warranted.
- A score of 400 to 999 carries an even higher plaque burden. Aggressive prevention is the appropriate course.
- A score of 1,000 or above demands immediate, aggressive intervention.
How to Read Your Percentile Rank
The report will include a second number: your percentile rank. This compares your score with those of other people of your age and gender.
For example, my score of 14 at age 61 put me in the 33rd percentile, meaning 33 out of 100 theoretical men my age would have had less coronary calcium, and 67 would have had more. If that same score of 14 had occurred at age 40, it would have placed me in the 90th to 95th percentile, worse than 90 to 95% of the age- and gender-matched cohort. Same absolute number, vastly different clinical significance.
The percentile tells you how far along the atherosclerosis progression you’ve traveled relative to your peers. But a common trap exists here: “normal” or 50th percentile might still indicate elevated risk.
In a society with high rates of hyperlipidemia, average doesn’t mean optimal. We’ve explored this theme in our discussion of healthy vs. normal cholesterol ranges, and the same logic applies.
Your calcium score percentile rank shows where you stand on the atherosclerosis continuum compared to others your age, but “average” in an unhealthy population isn’t a number you want to settle for.
Taking Action
The gift of this scan is knowledge. The next step is a careful conversation with your doctor about your cardiovascular risk profile, personal preferences, and a plan moving forward.
In my own case, the positive score prompted a statin that cut my LDL and ApoB by 30 to 35%. That kind of reduction, paired with lifestyle strategies like fish oil supplementation for cardiovascular risk and regular exercise, compounds over time. The benefit at 10 years is meaningful, and beyond 10 years, the risk reduction grows substantially as the baseline risk climbs with age.
Use the data from your calcium score test as the starting point for a risk-reduction conversation with your physician. Don’t let a positive score spiral into fear, and don’t let a zero score create false complacency.
Why Isn’t the Calcium Score Test Standard?
The calcium score test costs approximately $100 to $250 out of pocket, takes fewer than 10 minutes, and carries a radiation dose comparable to a mammogram. By most measures, it’s one of the most powerful cardiovascular screens available.
Insurance rarely covers it. Explaining why would require a separate article and leave nobody feeling cheerful. If you have the financial resources, this is one of the best places to put your healthcare dollar.
Today’s Takeaways
My story follows a familiar arc: a “healthy guy” with a normal-looking cholesterol panel who, without the calcium score test, would have missed the early signs of coronary artery disease. Half of all heart attacks happen to people in exactly that position.
The test is fast, inexpensive, and low-risk. The number it produces, your Agatston score, moves the conversation from statistical estimates to anatomical reality. It can guide cardiovascular risk management in a way no blood test alone can.
Ask your doctor about it. And if your doctor doesn’t bring it up, ask anyway. The rate-limiting step isn’t the test itself; it’s the awareness to order it.
At Banner Peak Health, we run calcium score testing as part of our standard cardiovascular risk assessment. Contact Banner Peak Health to discuss whether this screening makes sense for you.