To quote a bumper sticker, if you’re not confused, you’re not paying attention.
I say this often to patients who walk into my office asking about weight loss medications. The differences between tirzepatide and semaglutide are buried under overlapping brand names, competing advertisements, and social media noise. I’ve written about GLP-1 agonist side effects and cautions, and the most common request I receive now is a clear comparison.
The tirzepatide vs. semaglutide matchup isn’t as close as the marketing suggests. The data points in one direction, with cost and convenience as the only real counterweights.
Tirzepatide vs. Semaglutide: Brand Names
Before comparing tirzepatide vs. semaglutide, we need to untangle the naming confusion. I’m a physician, and I had to double-check this myself.
The same drug can carry different brand names depending on whether it’s prescribed for type 2 diabetes and A1C reduction or for weight management.
| Drug | Brand Name | Manufacturer | Approved Use | Form |
| Tirzepatide | Mounjaro | Eli Lilly | Type 2 Diabetes | Weekly injection |
| Tirzepatide | Zepbound | Eli Lilly | Weight Management | Weekly injection |
| Semaglutide | Ozempic | Novo Nordisk | Type 2 Diabetes | Weekly injection |
| Semaglutide | Wegovy | Novo Nordisk | Weight Management | Weekly injection |
| Semaglutide | Rybelsus | Novo Nordisk | Type 2 Diabetes | Daily oral tablet |
Mounjaro and Zepbound are the same drug (tirzepatide), made by Eli Lilly. Ozempic, Wegovy, and Rybelsus are all semaglutide, made by Novo Nordisk. Rybelsus is the only oral formulation available in either drug class.
How Tirzepatide and Semaglutide Work Differently
Our bodies aren’t simple if/then machines. They’re complex webs of hormones, receptors, and feedback loops. When we bring that perspective to the differences between tirzepatide and semaglutide, the mechanism becomes clearer.
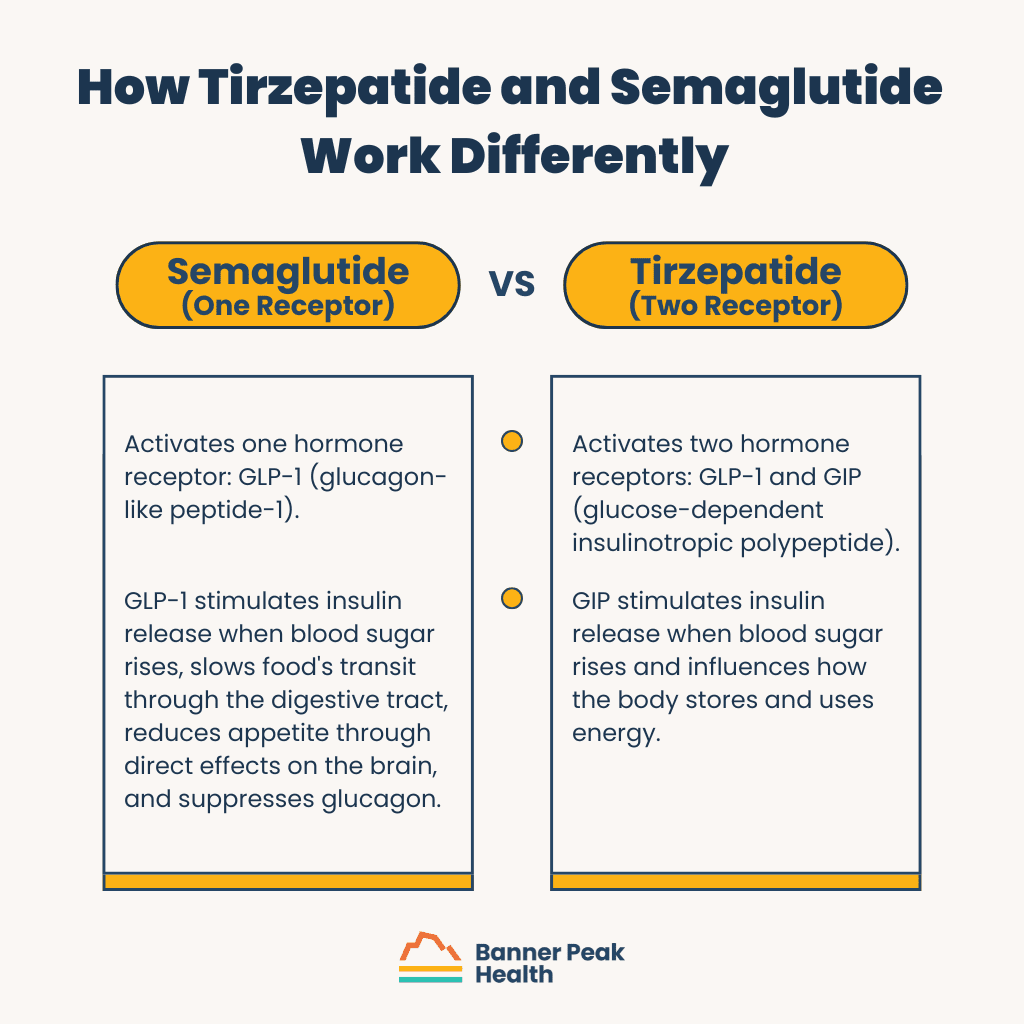
Semaglutide activates one hormone receptor: GLP-1 (glucagon-like peptide-1). The lower intestine releases GLP-1 after eating. It stimulates insulin release when blood sugar rises, slows food’s transit through the digestive tract, reduces appetite through direct effects on the brain, and suppresses glucagon (a hormone that raises blood sugar).
Tirzepatide activates two hormone receptors: GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). The upper intestine releases GIP in response to eating. GIP stimulates insulin release when blood sugar rises and influences how the body stores and uses energy.
That dual action touches on the same metabolic tug-of-war between building and breaking down tissue that governs how we gain or lose weight.
If one drug moves one lever and the other moves two levers, the two-lever drug will have a greater impact on the machine. The outcome data confirms this across nearly every measure.
Tirzepatide vs. Semaglutide for Weight Loss
The head-to-head data comes from the SURMOUNT-5 study, one of the longest trials directly comparing these two medications. The study enrolled patients with obesity (without diabetes) and followed them for 72 weeks.
Tirzepatide produced 20.2% weight loss compared to 13.7% with semaglutide, a 6.5-percentage-point gap. In actual pounds, patients on tirzepatide lost an average of 50 pounds, compared with 33 pounds with semaglutide.
Real-world data supports these findings. A study tracking 18,000 patients over 12 months confirmed tirzepatide patients lost 15.3% of their body weight, compared to 8.3% with semaglutide.
For anyone evaluating tirzepatide vs. semaglutide for weight loss, it’s important to explore what’s happening to body composition beyond BMI underneath those results.
Tirzepatide vs. Semaglutide for Blood Sugar and Heart Health
Weight loss is one piece of the picture. For patients managing type 2 diabetes, glycemic control and cardiovascular protection matter just as much.
The SURPASS-2 trial compared tirzepatide and semaglutide for blood sugar management. Tirzepatide at 15 milligrams reduced hemoglobin A1C by 2.3 percentage points, compared to 1.86 percentage points with semaglutide at one milligram.
More striking, 46% of tirzepatide patients reached near-normal blood sugar levels (A1C below 5.7%), versus only 19% on semaglutide. For patients already monitoring their glucose levels, that gap can mean the difference between medication dependence and metabolic freedom.
For cardiovascular health, the two medications offer comparable protection against heart attack, stroke, and cardiovascular death. Tirzepatide shows a slight edge in blood pressure reduction and cholesterol improvement, with HDL increasing by 7%–8% versus 4% with semaglutide. If you’ve been keeping an eye on your non-HDL cholesterol levels, those incremental gains can compound over time.
Across metabolic outcomes, the comparison between tirzepatide and semaglutide ends either in a tie or a tirzepatide advantage.
Tirzepatide vs. Semaglutide Side Effects
Both medications carry a high rate of gastrointestinal side effects: nausea, diarrhea, vomiting, and constipation. These symptoms are usually mild, and patients can manage them by gradually increasing the dosage over several weeks.
Tirzepatide, the more potent of the two, actually carries a lower incidence of GI side effects. In the SURMOUNT-5 study, only 2.7% of tirzepatide patients stopped treatment due to GI symptoms. Twice as many semaglutide patients had to discontinue for the same reason.
A separate concern applies to both medications: lean body mass loss. When the number on the scale drops, some of that loss comes from muscle and bone, not fat. Studies on GLP-1 agonists have shown that up to 39% of total weight loss can come from lean mass, a ratio worse than that of older weight-loss drugs.
Preserving muscle and bone matters more as we age, which is why pairing either medication with a resistance-training program is the best countermeasure I know of.
Today’s Takeaways
When a patient asks me about tirzepatide vs. semaglutide, the conversation is usually short. For weight loss, blood sugar control, cardiovascular markers, and tolerability, tirzepatide is the better drug across all measures. The data from SURMOUNT-5 and SURPASS-2 aren’t ambiguous.
Two factors can shift the calculus. The first is cost: Tirzepatide is more expensive, and insurance coverage varies. If financial access is a barrier, semaglutide remains an effective option with strong clinical evidence behind it.
The second is convenience. Semaglutide is the only one of these two drugs available as an oral tablet (Rybelsus). For patients who can’t tolerate injections, whether from needle aversion, localized skin reactions, or travel logistics that make managing metabolic health on the go more complicated, the oral route matters.
At Banner Peak Health, we evaluate every patient’s full clinical picture before recommending either medication. The right drug depends on your health goals, your metabolic profile, and your practical circumstances.
If you’re considering either option, contact us to schedule a visit. We’re happy to walk through the data together.