I’m not a basketball fan. That hasn’t stopped me from reaching for a basketball metaphor.
At 17, LeBron James appeared on the cover of Sports Illustrated, unprecedented attention for a high school junior. The hype panned out: number one NBA Draft pick, four NBA championships, four MVP awards, and the all-time NBA scoring leader.
Retatrutide appears to be the LeBron of weight loss drugs.
Phase 1 and Phase 2 trials are complete, and Phase 3 is ongoing. FDA approval remains several years out, but the data so far is striking enough that the drug made the cover of the New England Journal of Medicine before Phase 3 completion. For patients and physicians watching the field, retatrutide deserves attention alongside the current GLP-1 weight loss drugs.
What Is Retatrutide?
Retatrutide is a single peptide delivered as a once-weekly injection. Retatrutide is a triple agonist nicknamed “Triple G” for the three G-protein coupled receptors it targets at once: GIP, GLP-1, and glucagon.
Each hormone plays a role in how the body handles food, energy, and blood sugar. GIP and GLP-1 reduce food intake and improve insulin signaling. Glucagon receptor activation adds a third dimension that changes how the drug works at the metabolic level.
For background on the insulin and blood sugar side of this equation, see our blog post on hemoglobin A1C and blood sugar.
Why Retatrutide Adds Glucagon to the Equation
To grasp why retatrutide matters, look at what’s already on the market. Semaglutide targets GLP-1 alone. Tirzepatide targets GIP plus GLP-1.
Retatrutide adds the third agonist target, the glucagon receptor, which adds another mechanism for weight loss.
GLP-1 and GIP reduce food intake and improve insulin signaling, which helps with blood sugar control. Glucagon receptor activation operates on a different angle: it increases energy expenditure and promotes fat oxidation, the metabolism and burning of fatty acids in the liver.
The combined effect is potent: less food coming in, more calories burned, and active fat metabolism in the liver. This three-way mechanism is why the early retatrutide results have been so striking.
Readers tracking metabolic health may want to revisit our work on how to reset your metabolism.
The Phase 2 Retatrutide Trial Results
A quick primer on drug trials. Phase 1 tests safety in a small group. Phase 2 expands the sample, often with placebo control, and homes in on effective dosing. Phase 3 is the largest controlled trial and provides the data the FDA needs for approval.
Retatrutide’s Phase 2 results landed on the cover of the New England Journal of Medicine in 2023, before Phase 3 even finished. That fact alone speaks to the magnitude of what researchers saw.
The trial tested placebo against three retatrutide doses, including a maximum dose of 12 milligrams. At that 12-milligram dose, 100% of retatrutide participants lost more than 5% of body weight, 93% lost more than 10%, and 26% lost more than 30%.
Numbers of this magnitude are uncommon outside surgical interventions. The only other medical option producing this kind of weight loss is bariatric surgery. Weight loss curves had not plateaued at the 48-week trial stop point, so a longer trial could yield even larger results.
For context on what changes in body weight mean for health, see our discussion of BMI vs. body composition.
Retatrutide vs. Tirzepatide vs. Semaglutide
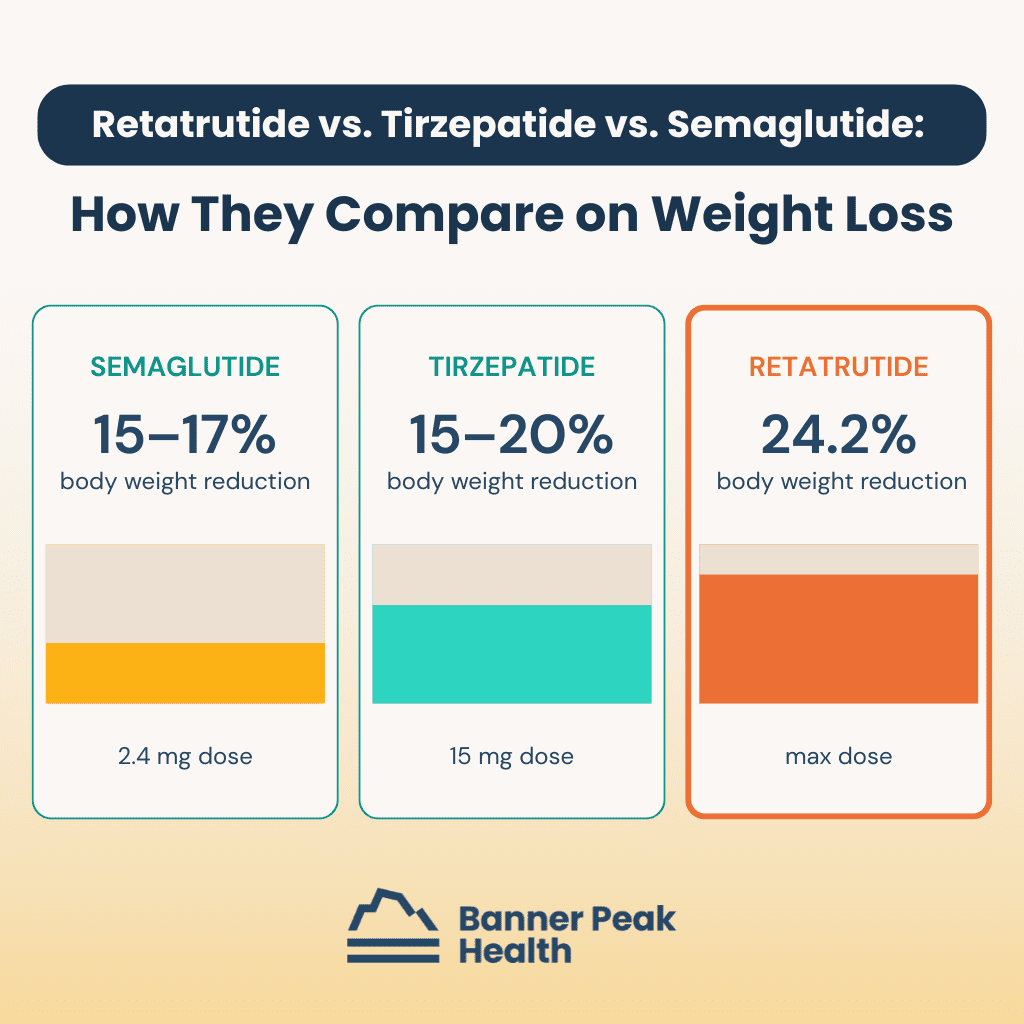
The comparison is what makes the early data so striking. Semaglutide at 2.4 milligrams (the dose used for weight loss) achieves a 15–17% reduction in body weight. Tirzepatide at 15 milligrams achieves 15–20%.
At the maximum dose, retatrutide achieved a 24.2% body weight reduction during the same trial period, the highest figure for any single agent.
These numbers aren’t apples-to-apples across separate trials, but the magnitude advantage is consistent: more receptor targets, more weight loss. The triple-agonist mechanism appears to produce the most potent weight loss yet observed with a single pharmacologic agent.
For readers interested in how the body’s weight regulation systems work, see our blog post about anabolism versus catabolism in weight loss.
Other Conditions Under Study With Retatrutide
The weight loss data was dramatic on its own. Other endpoints from the Phase 2 trial were similarly striking.
The drug reduced hemoglobin A1C by 2.2%, an industry-leading drop for this category. Systolic blood pressure dropped by nine mmHg. Triglycerides fell by 35%.
The most surprising finding from the retatrutide trial may have been the effect on liver fat: 86% of participants at the maximum dose had normal liver fat at the end of the study, with a mean reduction of 84%.
This matters for the growing population with MASLD (metabolic dysfunction–associated steatotic liver disease), a condition without good pharmacologic treatment until now. The ongoing Phase 3 trial will study retatrutide’s effects on obstructive sleep apnea, knee osteoarthritis, chronic kidney disease, cardiovascular progression, and type 2 diabetes.
Retatrutide Side Effects and the Discontinuation Concern
Every powerful drug has a cost. Retatrutide’s side effect profile lines up with the broader GLP-1 category, with gastrointestinal issues most common: nausea, vomiting, diarrhea, and constipation.
In the Phase 2 trial, up to half of retatrutide participants in the higher-dose groups reported these side effects. That rate is high but not out of line for the category. What concerned reviewers was the discontinuation rate, the share of participants who stopped taking the drug due to side effects.
Retatrutide showed a 17% discontinuation rate compared with 4% on placebo, roughly three times the 4.3–7.1% range seen in other GLP-1 medications.
This matters for what we call generalizability. Study participants tend to be healthier than the general patient population because exclusion criteria exclude comorbidities and older patients. They tend to be more dedicated than typical patients, the kind of people who volunteer for drug trials in the first place.
In the real world, with older patients and more health complications, the discontinuation rate will likely be even higher. Tolerability could be the deciding factor for individual patients considering retatrutide.
When Retatrutide Will Be Available
Merely being on the cover of NEJM won’t make retatrutide available on the market. Phase 3 trials need to finish, the data needs analysis and publication, and the FDA needs to grant approval. Clinical access remains several years away.
For patients in the Bay Area, we follow these developments closely. The team at our practice tracks emerging retatrutide research alongside the GLP-1 drugs already available, so our members have clarity on what’s working and what’s still in trials.
Today’s Takeaways
Retatrutide is the most exciting weight loss drug in the pipeline. The Phase 2 data shows weight loss approaching what previously required bariatric surgery, plus meaningful drops in hemoglobin A1C, blood pressure, triglycerides, and liver fat. The triple-agonist mechanism is new for the category.
The caveat is the 17% discontinuation rate, which suggests retatrutide may not be tolerable for the broader patient population.
If you’re following weight loss medications, retatrutide is worth tracking, and Phase 3 results over the next few years will tell us whether the early promise holds. Tools like continuous glucose monitoring help patients track their own metabolic baselines as these new options develop. To talk through what’s right for you, reach out to our practice.
Frequently Asked Questions About Retatrutide
When will retatrutide be available?
Retatrutide remains in Phase 3 trials. FDA approval requires Phase 3 completion, data analysis, peer review, and FDA evaluation. Clinical access is several years away.
How much weight loss does retatrutide produce?
In the Phase 2 trial at the 12-milligram dose, 100% of participants lost more than 5% of body weight, 93% lost more than 10%, and 26% lost more than 30%. Mean weight reduction reached 24.2% at 48 weeks, the highest figure published for any single weight loss agent.
How does retatrutide compare to Ozempic and Mounjaro?
On weight loss alone, retatrutide’s Phase 2 results exceeded the published numbers for semaglutide (Ozempic, Wegovy) at 15–17% and tirzepatide (Mounjaro) at 15–20%. The trade-off shows up in tolerability, with a discontinuation rate roughly three times that of other GLP-1 medications.
What are the side effects of retatrutide?
Gastrointestinal side effects are the most common: nausea, vomiting, diarrhea, and constipation. Up to half of participants in higher-dose groups reported these in the Phase 2 trial. The 17% discontinuation rate is the highest concern, roughly three times the 4.3–7.1% range for other GLP-1 medications.
